Understanding
Friedreich Ataxia

mFARS measures FA progression by evaluating
multiple aspects of a patient's neurological function
mFARS measures1
The mFARS is made up of 4
sections that focus on
functional abilities
The mFARS is scored on a scale of 0 to 93, with higher scores indicating more severe physical impairment.1
mFARS measures1
Lower limb coordination
Assessed Function: Coordination of legs and feet
Example Assessments and Scoring: Heel-along-shin slide, Heel-to-shin tap, 16 points total
Clinical Extrapolations of Possible Effects on Patient Abilities: Closely related to upright stability, also an important contributor to decline in ambulatory patients.2 Affects activities like putting on socks and shoes.
Upright stability
Assessed Function: Sitting, standing, and walking
Example Assessments and Scoring: Sitting posture, Stance, Gait, 36 points total
Clinical Extrapolations of Possible Effects on Patient Abilities: Assessment of individual ambulatory ability. Affects activities like walking, sitting in a car, standing in a line, and showering.
Upper limb coordination
Assessed Function: Fine motor coordination
Example Assessments and Scoring: Finger to finger, Nose to finger, Dysmetria, 36 points total
Clinical Extrapolations of Possible Effects on Patient Abilities: Ability to complete activities of daily living, such as getting dressed, eating, brushing teeth, typing, pointing, reaching, and turning a doorknob.
Bulbar function
Assessed Function: Speech clarity and strength and volume of coughing
Example Assessments and Scoring: Forceful cough, speech, 5 points total
Clinical Extrapolations of Possible Effects on Patient Abilities: Affects the ability to communicate clearly. Patients may also be at increased risk for respiratory infection.3
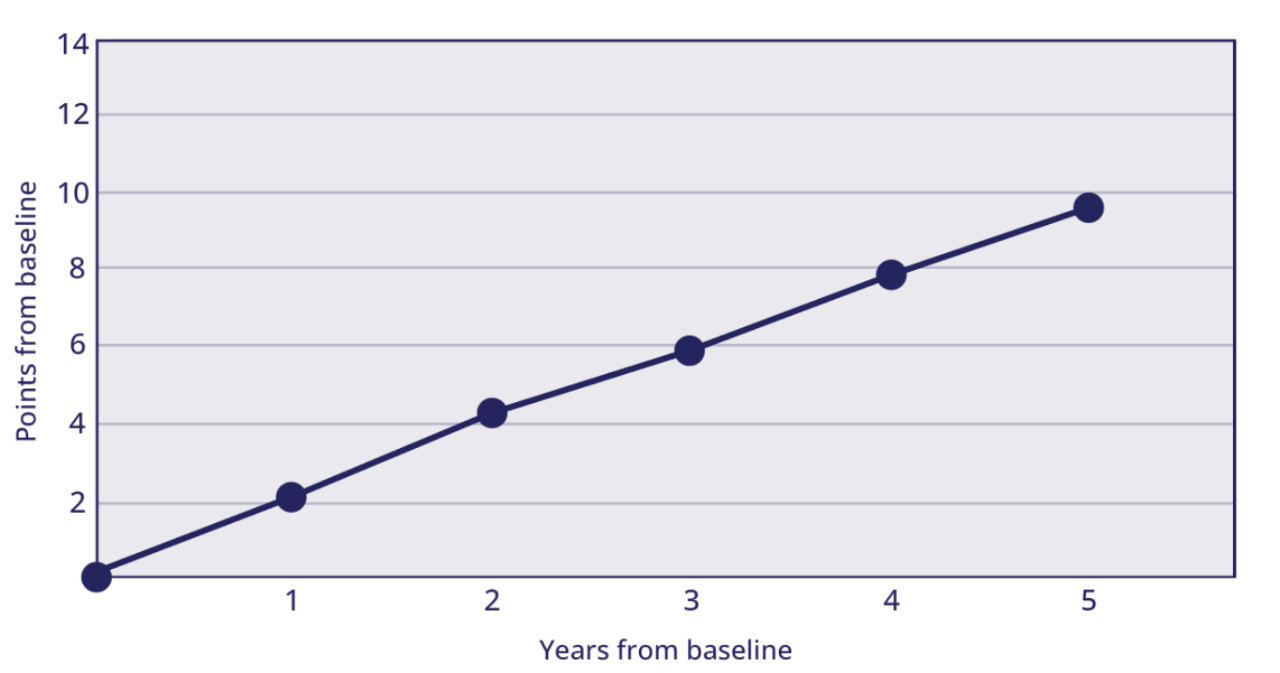
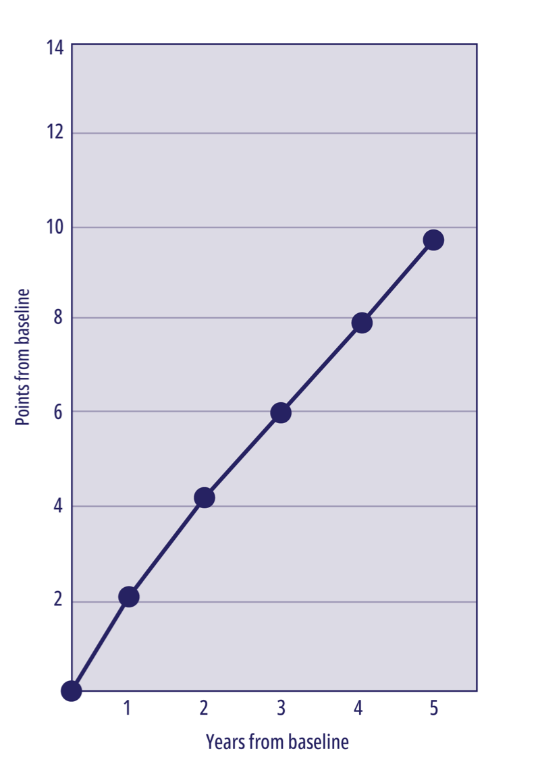
As FA progresses, a patient’s mFARS
score will worsen (increase)1,4
A large longitudinal natural history study of untreated patients found that FA progresses on average ~2 points per year.4
Mean change from baseline in mFARS4
It is important to discuss with patients that changes in mFARS can signal functional
decline, which may impact their ability to perform daily activities1,4